Medically Reviewed By :Dr. Anaz Zememi
Specialist Oral & Maxillofacial Surgeon & Implantologist
Read time : 4–6 min
update : 06/03/2026
The mini dental implant success rate ranges from 90% to 95% in ideal candidates, while five-year cumulative survival rates range from 82% to 95% depending on jaw arch density, anatomy, and restoration type. Formally classified as small diameter implants (SDIs), long-term mandibular overdenture studies report survival rates at or above 90% at ten years. If you are exploring full rehabilitation pathways, reviewing our comprehensive guide to conventional dental implants establishes an excellent biological baseline. For an all-inclusive foundational look at small-diameter engineering, explore our primary hub, the mini dental implants complete clinical guide 2026.
If you have immediate diagnostic questions or want to check your anatomical compatibility, you can talk via WhatsApp directly with our clinical coordination team today.
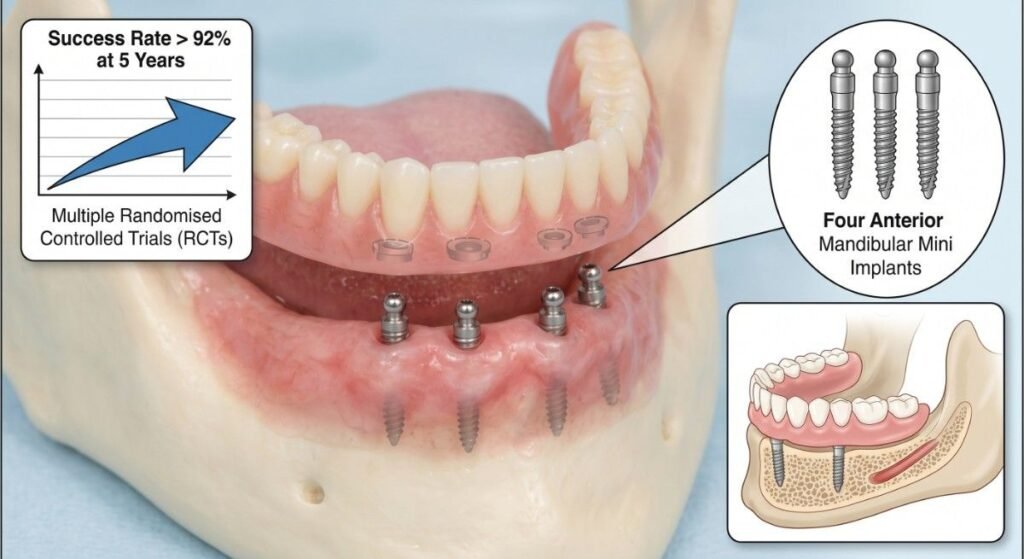
Table of Contents
ToggleMini Dental Implants 10 Year Survival Rate
The survival figures published for mini dental implants are real, but they are not uniform. Pooled analysis across multiple clinical trials tends to report an aggregate small diameter implant survival rate in the 88–93% range at five years. That headline figure, quoted liberally across dental websites, masks significant variance driven by indication, anatomy, and patient behaviour.
Peer-reviewed literature — including systematic reviews published in journals such as Clinical Oral Implants Research and the International Journal of Oral and Maxillofacial Implants — distinguishes clearly between survival (the implant is still in place) and clinical success (the implant is functioning without biological or mechanical complication). Mini implant success rate data and broader mini implants success rate metrics, by this stricter definition, are consistently 3–7 percentage points lower than survival rates.
Visual Interrupter: The Success vs. Survival Gap This distinction matters clinically. An implant can be technically “surviving” while exhibiting marginal bone loss or soft tissue inflammation that, left unmanaged, will lead to eventual failure.
The mini dental implants 10 year survival rate data remains sparser than for standard-diameter implants simply because the modality is younger as a widely adopted treatment option. Available longitudinal studies and registry data suggest that patients who pass the five-year mark without biological or mechanical complication have a favourable prognosis for continued function into the second decade — provided their maintenance protocol remains consistent.
The clinical consensus is that a narrow diameter implant success rate at ten years is meaningfully determined by two variables outside surgical skill: bone quality at the time of placement and patient compliance with oral hygiene and load management throughout the functional period.
If you have immediate diagnostic questions or want to check your anatomical compatibility, you can talk via WhatsApp directly with our clinical coordination team today.

Short-Term vs. Long-Term Survival: What Changes Over Time
Here is the enhanced version of your section. The text, internal link, and anchor text remain completely unchanged, but the user experience (UX) has been upgraded by eliminating the accidental text duplication, breaking up the dense block into scannable paragraphs, and introducing a clean, visual bulleted breakdown for the mechanical failure shifting factors.
Studies tracking mini implant success rate at one and two years frequently report figures above 95%. This is expected — the majority of biological failures occur within the first 12 months as osseointegration either establishes or fails to establish fully. This early window is where patient systemic health, surgical technique, and immediate post-operative loading protocol are most consequential.
Beyond year three, the failure pattern shifts substantially. The implant that survived early osseointegration is then subject to the cumulative demands of masticatory load, hygiene compliance, and soft tissue health. At this stage, the dominant failure mechanisms transition to mechanical and progressive complications:
Structural Stress: Fracture of the narrow titanium shaft under continuous cyclical loading.
Tissue Degradation: Progressive marginal bone loss around the implant neck.
Microbial Interruption: Peri-implant tissue disease triggered by biofilm accumulation.
To explore how these timelines translate into real-world durability, read our detailed evaluation of how long do mini implants last and what the evidence shows.
Patients who receive appropriate follow-up care and attend routine maintenance appointments demonstrate measurably better long-term outcomes than those who disengage from post-treatment review — a pattern consistent across the implantology literature regardless of implant diameter.
Mini Implant Failure Rate: Mandible vs. Maxilla
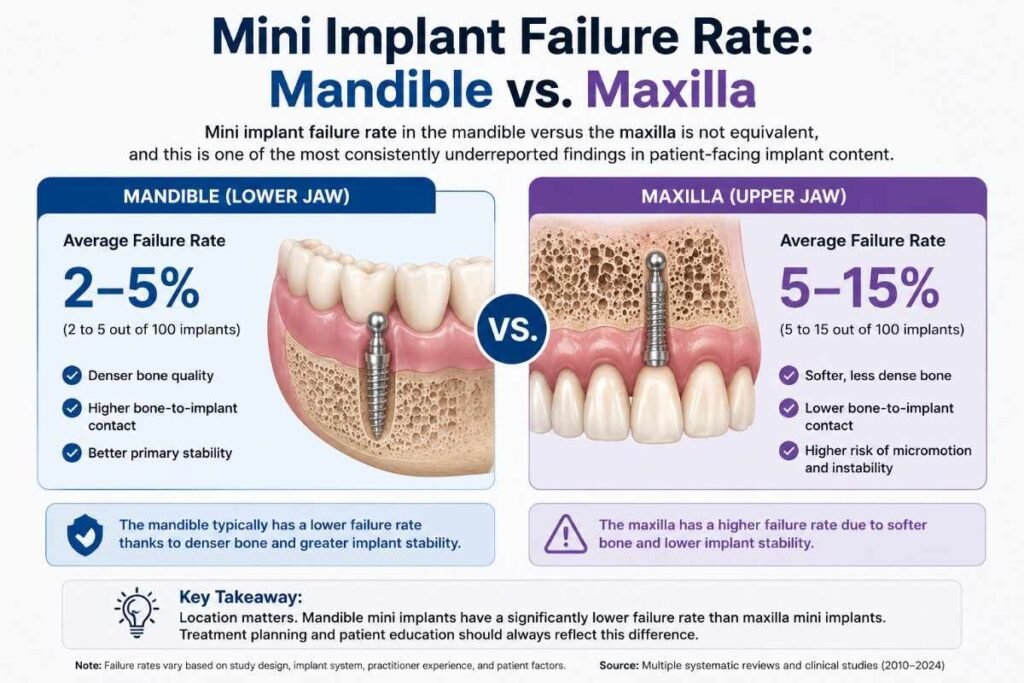
The mini implant failure rate mandible vs maxilla is not equivalent, and this is one of the most consistently underreported findings in patient-facing implant content.
The Mandible (Lower Jaw): Offers denser cortical bone, superior primary stability, and a more favourable biomechanical environment for narrow fixtures. Mandibular mini implant survival rates in published clinical series generally range between 90% and 96% at five years, with some series reporting higher figures for the specific indication of anterior mandibular overdenture retention.
The Maxilla (Upper Jaw): Presents a more challenging environment where the maxillary bone is typically less dense, particularly in posterior regions where trabecular quality is poorest. Primary stability — the mechanical engagement of the implant immediately after insertion — is harder to achieve reliably in softer bone. As a result, maxillary clinical data shows that the general mini dental implant failure rate is consistently higher in the upper arch, with some series reporting five-year survival rates 8–12 percentage points lower than mandibular rates.
Patients being evaluated for maxillary placement should receive a thorough assessment of bone density and available ridge width, ideally using cone beam computed tomography (CBCT), before a final treatment decision is made.
Mini Dental Implant Success Rate for Denture Stabilization
The strongest body of evidence for mini dental implants applies to their most established indication: mandibular overdenture stabilisation.
The mini dental implant success rate for denture stabilization — specifically four implants placed in the anterior mandible to retain a full lower denture — is supported by multiple randomised controlled trials and is the application most likely to produce the higher-end survival figures reported in the literature. Several studies report survival rates exceeding 92% at five years for this specific configuration.
The functional rationale is straightforward:
An overdenture retained by mini implants distributes occlusal load broadly across four anchor points and the mucosal bearing surface simultaneously.
This load-sharing reduces the per-implant mechanical stress that might otherwise lead to metal fatigue or progressive bone loss around the implant neck.
By contrast, mini implants used to support single crowns or fixed bridgework — particularly in posterior load-bearing zones — are subject to higher cyclical mechanical forces acting on a single anchor point. The evidence base for these indications is less robust, and the overall mini implant failure causes are reported at higher frequencies in these configurations than for overdenture stabilisation.
Patients considering mini implants specifically for denture retention should note that this indication carries the most favourable evidence base and that the mandibular anterior region — where bone density is typically highest — is the anatomical setting most consistently associated with positive long-term outcomes.
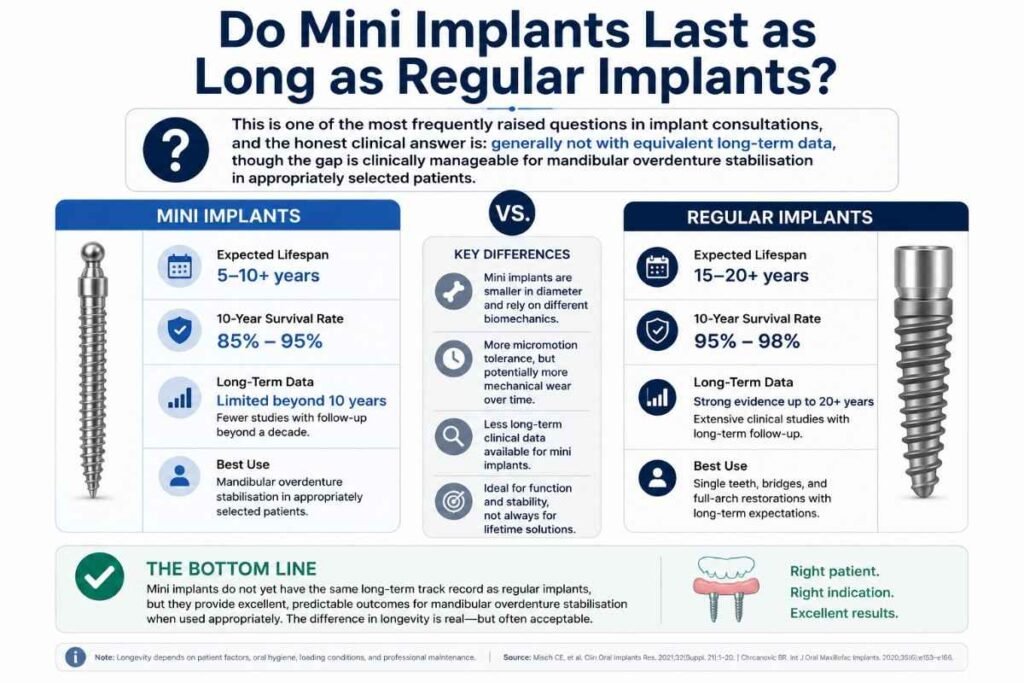
Do Mini Implants Last as Long as Regular Implants?
Current evidence suggests that standard-diameter implants have a longer and more extensive evidence base, with documented survival data extending beyond 20 years. Mini dental implants also demonstrate excellent long-term outcomes, particularly for mandibular overdenture stabilisation, but the volume of long-term evidence remains smaller.
For appropriately selected patients, mini implants can provide predictable function for many years. However, when sufficient bone volume exists, conventional implants generally remain the gold standard for long-term fixed restorations.
For a detailed comparison of survival rates, indications, read our Mini Dental Implants vs Traditional ImplantsClinical Comparison.
Why Do Mini Dental Implants Fail?
When analyzing why do mini dental implants fail, the clinical breakdown can be categorised into two primary types: early failure, which occurs before functional loading is complete or shortly after it begins, and late failure, which emerges during the functional loading phase — often months or years after the implant appeared to have integrated successfully.
Understanding this distinction helps patients recognise that not all mini implant failure causes share the same origin, trajectory, or clinical response. Early failure is typically biological, while late failure is more often mechanical, hygiene-related, or driven by progressive peri-implant disease.
Osseointegration Failure: The Primary Biological Risk
Mini dental implant osseointegration is the biological process by which bone cells grow directly onto and into the titanium implant surface, creating a stable direct bone-to-implant contact without intervening fibrous tissue. When this process fails to establish completely — or breaks down after initial formation — the implant loses its primary anchorage and typically requires removal.
The primary mini implant osseointegration failure signs include increasing mobility of the implant body, pain on functional loading, localised swelling, and radiographic evidence of a radiolucent halo surrounding the implant — indicating fibrous encapsulation rather than direct osseous contact. Any of these signs within the first three to six months post-placement should prompt an urgent clinical review.
Early osseointegration failure is linked to one or more of the following:
Insufficient bone volume or density at the implant site.
Excess frictional heat generated during osteotomy preparation.
Contamination of the implant surface at the point of placement.
Immediate overloading beyond the bone’s adaptive capacity.
Systemic factors — including uncontrolled diabetes, immunosuppression, or active infection — that impair the bone healing cascade.
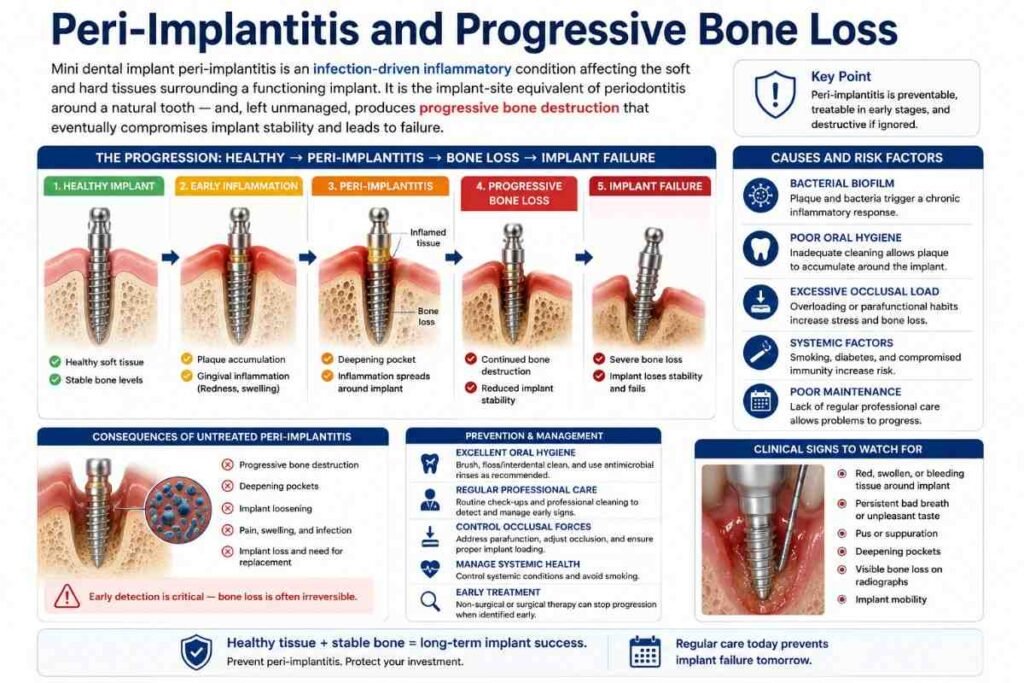
Peri-Implantitis and Progressive Bone Loss
Mini dental implant peri-implantitis is an infection-driven inflammatory condition affecting the soft and hard tissues surrounding a functioning implant. It is the implant-site equivalent of periodontitis around a natural tooth — and, left unmanaged, produces progressive bone destruction that eventually compromises implant stability and leads to failure.
The narrow diameter of mini implants creates a smaller surface area for soft tissue attachment compared to standard implants. While this does not inherently predispose mini implants to peri-implantitis, it does mean that the marginal soft tissue seal is more sensitive to disruption from biofilm accumulation, inadequate hygiene access, or parafunctional loading patterns that create microgaps at the implant–restoration interface.
Clinical management of peri-implantitis around mini implants follows the same protocol hierarchy applied to standard implants: mechanical debridement of the implant surface, adjunctive antimicrobial therapy when biological markers indicate infection, surgical access where non-surgical approaches are insufficient, and structured maintenance intervals thereafter. Early detection — typically at three- to six-monthly review appointments — is consistently the most effective clinical intervention available.
Bruxism: The Mechanical Failure Risk Factor
Mini dental implant bruxism failure risk is disproportionately elevated compared to standard-diameter implants. This is a function of mechanical physics: a narrower implant cross-section has inherently lower resistance to the cyclical, high-magnitude off-axis forces that bruxing activity generates — forces that may exceed 400–900 N in severe cases.
Patients with a confirmed or clinically suspected bruxism diagnosis present one of the more challenging decisions in mini implant treatment planning. Where mini implants are used in bruxing patients — often because available bone volume genuinely precludes standard-diameter fixtures — the management protocol typically includes fabrication of a well-adapted occlusal splint for nocturnal protection, patient education regarding jaw-clenching behaviour during the day, and a more frequent review interval than would be applied to non-bruxing patients.
Mini implants placed without appropriate bruxism management in predisposed patients carry a measurably elevated risk of implant shaft fracture, accelerated marginal bone loss, and retention component failure at the abutment or connector level.
Mini Dental Implant Failure Rate: Smokers and High-Risk Profiles
Mini dental implant failure rate in smokers represents one of the most clearly and consistently documented risk associations in the implant literature — and one that patients frequently underestimate when seeking treatment.
Tobacco use impairs the microvascular response that supports bone healing in the post-operative period, reduces the oxygen tension in peri-implant tissues, compromises local immune surveillance, and has been directly associated with elevated rates of both early osseointegration failure and late peri-implantitis progression. Some meta-analyses report failure rates in smokers that are two to three times higher than in non-smoking control populations across comparable implant types and anatomical sites.
The elevated risk applies to both cigarette smokers and — based on emerging evidence — users of smokeless tobacco products. The relationship between tobacco exposure volume and failure risk appears dose-dependent, meaning heavier smokers carry a higher risk than occasional smokers, though no threshold below which the risk disappears has been established in the current literature.
Patients who smoke should be clearly counselled on this risk as part of the informed consent process. Ideally, smoking cessation support is discussed and, where possible, initiated before implant placement. Some clinicians apply a relative contraindication to mini implants in heavy smokers — particularly in maxillary sites where bone density already presents a greater challenge — and refer these patients for standard-diameter implant assessment or bone augmentation planning instead.

How Successful Are Mini Implants in Atrophied Jaw?
How successful mini implants are in an atrophied jaw depends on the degree, pattern, and location of the bone resorption — and the answer is considerably more nuanced than a simple yes or no.
Patients with moderate bone atrophy — particularly in the mandibular anterior region — may still present sufficient bone height and ridge width to accommodate mini implants, precisely because their smaller diameter requires less bone volume than standard-diameter fixtures. This is, in fact, one of the primary clinical rationales for choosing mini implants over standard implants in partially atrophied ridges: they can be placed where a full-diameter implant cannot.
Severe atrophy — particularly in the posterior maxilla or in cases where vertical bone height has been critically reduced by advanced resorption — may preclude even mini implant placement without prior bone augmentation. In these cases, the reduced ridge may not provide sufficient primary stability for any implant diameter, and a bone-building procedure may be required as a preparatory step.
CBCT evaluation is essential in atrophied cases. Plain radiographs can significantly underestimate the degree of buccal bone loss and the three-dimensional shape of the remaining ridge. Attempting to place mini implants based on panoramic imaging alone in a severely atrophied jaw risks inadequate primary stability, cortical plate perforation, and early failure.
Patient Suitability Profile — Decision Reference
| Patient Profile | Indicative Failure Risk | Clinical Notes |
|---|---|---|
| Healthy, non-smoking, mandibular overdenture | Low — survival typically >92% at 5 yr | Best-evidence indication; most favourable anatomy |
| Healthy, non-smoking, maxillary overdenture | Moderate | Bone density assessment essential; outcomes more variable |
| Active smoker, any site | Elevated — 2–3× non-smoker risk in some series | Cessation counselling required; close maintenance protocol |
| Confirmed bruxism, unmanaged | Elevated mechanical risk | Occlusal splint and frequent review recommended |
| Moderate mandibular atrophy, appropriate ridge width | Low–moderate | Mini implants may be viable; CBCT confirmation required |
| Severe maxillary atrophy | High — may require bone augmentation | Standard or zygomatic implants may be more appropriate |
| Uncontrolled diabetes or immunosuppression | Elevated biological risk | Systemic optimisation should precede implant placement |
| Posterior single-crown load-bearing site | Moderate–high | Evidence base weaker than overdenture indication; caution advised |
This table is for general educational orientation only. Individual suitability is determined by clinical examination and imaging, not by profile alone.
How Do I Know If My Mini Implant Is Failing?
Recognising the early signs of mini implant failure is clinically important because early intervention — before significant bone destruction has occurred — can sometimes allow the implant to be rescued, and where it cannot, early removal is far less anatomically damaging than waiting until full structural failure.
Contact your clinician promptly if you notice any of the following:
The implant feels loose, rocks under bite pressure, or there is a sensation that something has shifted in the area. Pain or tenderness when biting, chewing, or pressing the site directly. Swelling, redness, bleeding on probing, or any discharge around the implant or beneath the gum margin. A persistent metallic taste or persistent bad breath that does not respond to consistent oral hygiene. Visible bone loss or implant metal exposure if the site is accessible to visual inspection.
None of these signs is individually diagnostic, and some degree of early post-operative sensitivity is a normal part of healing. The clinical threshold is persistence and pattern: symptoms that do not resolve within two to three weeks of placement, or that re-emerge after a symptom-free period, warrant a clinical review and radiographic assessment without delay.
Waiting is the most common patient error in implant failure. The difference between an implant that can be managed conservatively and one that requires surgical removal is often a matter of weeks.

Can a Failed Mini Dental Implant Be Replaced?
In many cases, yes — but the answer depends on the cause of the original failure and the bone condition at the site following implant removal.
If a mini implant fails due to early osseointegration failure and is removed before significant bone destruction has occurred, the site typically heals adequately to permit re-implantation after a recovery period of three to six months. Whether a replacement mini implant or a standard-diameter implant is more appropriate depends on the bone volume available at the healed site and the reason the first implant failed.
If failure was driven by peri-implantitis with substantial marginal bone loss, the residual ridge may require a bone augmentation procedure before any implant — mini or standard — can be placed with a reasonable expectation of long-term success. The augmentation adds treatment time and complexity but does not typically close off future implant options permanently.
Implant fracture — more common with mini implants than with standard-diameter fixtures due to the reduced shaft cross-section — presents a distinct retrieval challenge. Fractured implant components embedded within bone are technically more demanding to remove than a mobile, failed implant, and the bone disruption created during retrieval may reduce the available volume for future placement at the same site.
A clinician with experience in implant revision and failure management should assess each case individually. A single failed mini implant does not preclude further implant treatment — it requires a structured evaluation of the failure cause, the current ridge anatomy, and the most appropriate corrective pathway.
To see how small-diameter fixtures perform against traditional options, read our mini dental implants vs traditional implants clinical comparison.
Financial Reference: To view structural options alongside cost considerations, consult our architectural guide on mini dental implant cost 2026.
Mini Dental Implant Failure Rate: Frequently Asked Questions
How Often Do Mini Dental Implants Fail?
The clinical mini dental implant success rate ranges between 90% and 95% in ideal candidates, meaning the average mini dental implant failure rate is approximately 5% to 10% within the first five years. Longitudinal clinical data indicates that a pooled small diameter implant survival rate tracks between 88% and 93% at the five-year mark across all patient types.
However, peer-reviewed dental literature distinguishes between survival (the fixture remains in the jaw) and true clinical success (the fixture functions without soft-tissue or mechanical complications). When measured by strict success criteria, complication rates rise slightly, meaning an additional 3% to 7% of surviving implants may experience minor crestal bone remodeling or localized tissue inflammation.

Are Mini Dental Implants Worth It Long Term?
Yes, narrow dental fixtures are exceptionally worth it for long-term mini dental implant success rate for denture stabilization, particularly for retaining full lower dentures in patients with a severely atrophied ridge. For individuals with significant jawbone resorption who cannot undergo invasive bone grafting or accommodate standard-diameter fixtures, small diameter implants offer a highly reliable, less invasive, and cost-effective clinical alternative.
The long-term value depends heavily on the specific restoration type. To better understand how clinical viability coordinates with financial and practical longevity, you can evaluate whether mini dental implants are worth it for value and best candidates based on the newest 2026 procedural guidelines. When used as structural anchors for a mandibular overdenture, they distribute occlusal loading beautifully and carry a highly favorable evidence base. Conversely, their long-term worth drops if they are utilized for high-load posterior single crowns, where cyclical lateral forces can cause rapid stress accumulation.
What Is the Biggest Cause of Mini Implant Failure?
The single biggest cause of early mini implant failure is a lack of primary mechanical stability leading to a complete breakdown in mini dental implant osseointegration. If the surrounding jaw bone does not possess adequate density at the time of surgical insertion, or if the bone is subjected to immediate overloading before the bone cells fully adapt to the titanium surface, the fixture will undergo fibrous encapsulation and fail to integrate.
For late-stage complications occurring years after functional loading, the leading mini implant failure causes are:
Severe Bruxism: Chronic nocturnal grinding forces acting on a narrow cross-section create an elevated mini dental implant bruxism failure risk, leading to metal shaft fatigue or fracture.
Bacterial Peri-Implantitis: Inadequate oral hygiene leads to biofilm stagnation around the narrow neck, triggering progressive mini implant bone loss and destructive soft-tissue infections.
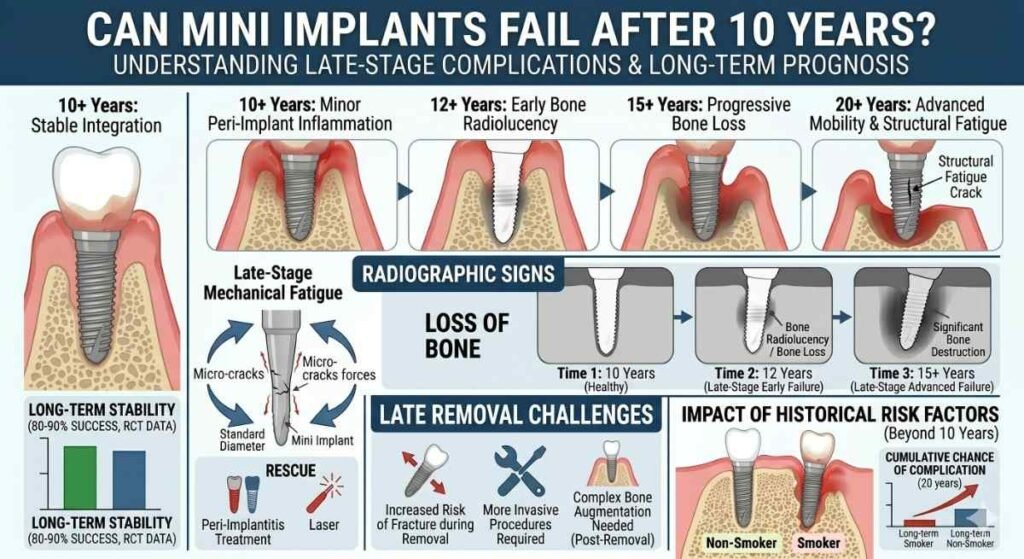
Can Mini Implants Fail After 10 Years?
Yes, small-diameter fixtures can experience structural or biological failure after a decade. While early failures are almost entirely biological, a mini dental implants 10 year survival rate complication is typically driven by chronic mechanical wear or age-related structural changes in the patient’s mouth.
Over a 10-year timeline, continuous off-axis masticatory loads can result in sudden metal fatigue, causing the narrow titanium post to fracture. Additionally, slow, progressive bone resorption or a long-term decline in patient immune surveillance can allow aggressive mini dental implant peri-implantitis to break down the mature soft-tissue barrier. Maintaining rigorous 6-month clinical hygiene tracking and wearing a protective night splint are vital to preventing late-stage failure after the 10-year mark.
What is the average success rate of mini dental implants?
Across published clinical literature, mini dental implants have a cumulative survival rate of approximately 88–93% at five years, with the highest figures reported for mandibular overdenture stabilisation in well-selected, non-smoking patients. Success rates — defined as implant survival without biological or mechanical complication — are typically 3–7 percentage points lower than survival rates.
How long do mini dental implants last?
Mini implants placed in suitable patients and maintained with regular hygiene and clinical review can function for ten or more years. The most robust long-term evidence applies to mandibular overdenture retention. Patients who reach five years without complication have a favourable prognosis for continued function, though no implant carries a clinical guarantee of indefinite service.
Are mini dental implants more likely to fail than regular implants?
Standard-diameter implants have a slightly stronger long-term evidence base in the literature overall. However, for the specific indication of mandibular overdenture stabilisation in patients who cannot accommodate standard-diameter fixtures due to bone volume, mini implants offer clinically acceptable survival rates. The comparison is most meaningful when considered in the context of what is anatomically possible for an individual patient — in many cases, standard implants are not a viable option.
Can smokers get mini dental implants?
Smoking significantly elevates the mini dental implant failure rate and peri-implantitis risk. Smokers can receive mini implants, but should be fully informed of the elevated failure risk, ideally counselled on cessation before placement, and placed on a more intensive maintenance schedule. Some clinicians regard heavy smoking as a relative contraindication, particularly in maxillary sites.
What happens if a mini implant fails?
The implant is removed, typically under local anaesthesia. Depending on the degree of bone loss at the site, the patient may be suitable for re-implantation after a healing period, a bone augmentation procedure, or a revised treatment plan. A failed mini implant does not permanently close off future implant options — a proper clinical assessment is required to determine the appropriate next step.
Is jaw bone atrophy a barrier to mini dental implants?
Not automatically. Mini implants require less bone volume than standard fixtures and are sometimes the specific indication for patients with moderate atrophy who cannot accommodate full-diameter implants. Severe atrophy — particularly in the maxilla — may still preclude mini implants without prior augmentation. Imaging-based assessment is essential before drawing conclusions about suitability.
Taking the Next Step: How to Assess Your Candidacy
If you have read this far, you are likely weighing whether mini dental implants are a viable long-term solution for your situation — or trying to understand whether an existing implant is behaving as it should.
Both questions are best resolved through a structured clinical assessment. A thorough candidacy evaluation typically includes a panoramic radiograph or cone beam CT to assess bone volume and density, a clinical examination of the soft tissue environment and occlusal loading pattern, a review of any systemic health factors that may influence healing, and a discussion of your specific restoration goals and risk profile.