Medically Reviewed by Dr. Anas Zemzemi | Updated for 2026 May Clinical update
Most patients reach this question after their dentist has already recommended a bridge. The material decision — zirconia or porcelain — can feel overly technical. But it comes down to three things: where the bridge sits in your mouth, whether you prioritise strength or the finest possible aesthetic nuance, and how your bite behaves.
Both zirconia dental bridges and porcelain bridges can restore missing teeth and look natural. The difference between zirconia and porcelain lies in how they are constructed, how they perform under pressure, and how they age alongside your gum tissue.
For a full foundation on how dental bridges work and the types available, see our separate guide. If you are still deciding between restorative options, you may also want to compare implants vs bridging of teeth to see which treatment lasts longer for your specific case.
Clinical Assessment: Unsure which material suits your bite? You can share your question with the Kristal Clinic team via WhatsApp for a remote clinical evaluation before making your decision.
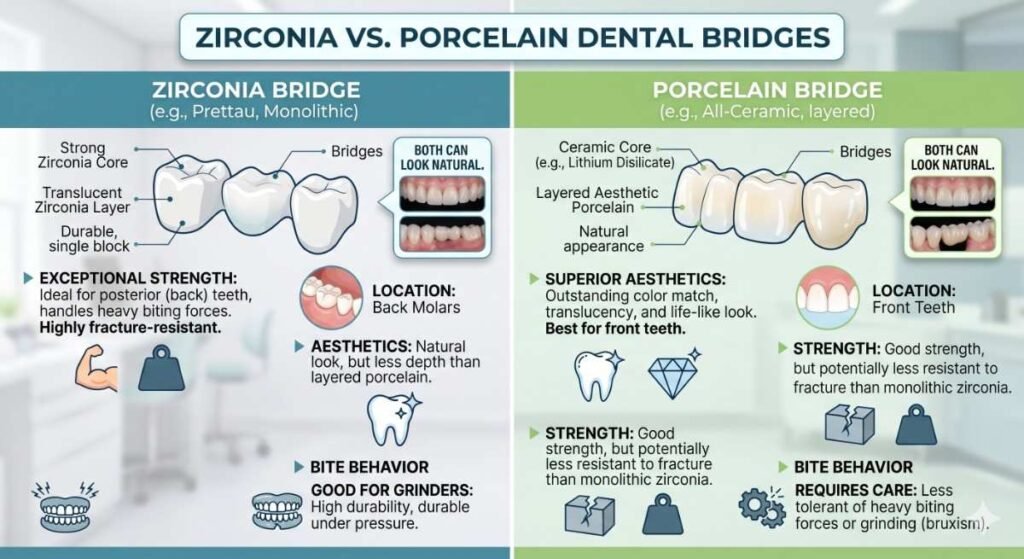
Table of Contents
Toggle🔍 Quick Answer — Zirconia Dental Bridge vs Porcelain
Zirconia dental bridges are stronger, more fracture-resistant, and more biocompatible than porcelain. They are the preferred choice for most patients — particularly for back teeth, patients with bruxism, and those with metal sensitivities. Porcelain bridges offer slightly finer translucency, making them relevant in specific aesthetic cases for highly visible front teeth.
For the majority of patients, zirconia is the more reliable long-term material. The question is not which material is universally better — it is which material suits your specific clinical situation.
If you are evaluating your bridge material options before booking, you can share your dental X-ray or CBCT scan with the Kristal Clinic clinical team for a no-cost remote assessment.
What Is the Difference Between a Zirconia and Porcelain Dental Bridge?
The difference between zirconia and porcelain in restorative dentistry is primarily a question of material science — not just aesthetics. Both materials can construct a fixed bridge. How they are made, and how they behave inside your mouth over time, determines which suits your case.
What Is Zirconia Made Of?
Zirconia — formally known as zirconium dioxide (ZrO₂) — is a high-strength advanced ceramic. It is milled from a solid block using CAD/CAM (computer-aided design and manufacturing) technology, producing a restoration with exceptional structural precision. Modern variants — including monolithic zirconia and translucent zirconia — have been specifically engineered to improve optical appearance without sacrificing structural strength. Zirconia is entirely metal-free and has been in clinical use for dental restorations for over two decades.
What Is Porcelain Made Of?
Dental porcelain is a glass-ceramic that mimics the optical properties of natural tooth enamel. It can be used alone as an all-ceramic bridge, or fused to a metal substructure for added support — a construction known as porcelain-fused-to-metal (PFM). All-ceramic porcelain is valued for its lifelike translucency. PFM has served as the standard for decades, though zirconia-based materials have largely replaced it in modern restorative practice.

Strength and Durability: Which Handles More Pressure?
This is the most clinically significant difference between the two materials.
Zirconia resists fracture far better than porcelain. It can tolerate occlusal force — the biting and chewing pressure your teeth generate — with a flexural strength that ranges between 900 and 1,200 megapascals (MPa) depending on the grade. All-ceramic porcelain sits substantially lower, typically between 100 and 400 MPa depending on construction method.
For everyday clinical decisions: zirconia is far less likely to chip or crack under sustained biting pressure. Porcelain, while durable relative to natural enamel, is more brittle. It is particularly vulnerable to fracture from heavy loading, bruxism (teeth grinding), or uneven bite patterns.
Why Zirconia Performs Better for Molars and Back Teeth
Your back teeth generate the highest chewing force in your mouth. A zirconia bridge for back teeth is the clinical standard for this reason — the material’s hardness means it tolerates repeated loading without micro-fracturing over time.
If you clench or grind your teeth, your clinician will almost always recommend zirconia over porcelain for posterior restorations. For long-span bridges replacing multiple adjacent teeth, the structural advantage of zirconia becomes even more pronounced.
For a detailed breakdown of how long each material lasts, see our guide on zirconia dental bridge lifespan and full-arch options.
Aesthetics: Which Looks More Natural — Zirconia or Porcelain?
What looks more natural — zirconia or porcelain? The honest answer is: it depends on which generation of zirconia is being used and the quality of the dental laboratory producing it.
Traditional zirconia was opaque — it lacked the depth and internal translucency of natural teeth, which made it a weaker aesthetic choice in its early clinical years. That has changed substantially. Translucent zirconia — engineered with a more glass-like internal structure — can now replicate the layered appearance of natural enamel to a degree that most patients, and many clinicians, cannot distinguish from a high-grade porcelain restoration under normal conditions.
Porcelain still holds a narrow aesthetic advantage in very specific situations. Its capacity to reproduce the finest gradients of colour and the optical depth of natural enamel remains unmatched in extreme aesthetic cases — particularly for patients with very light, highly translucent natural teeth where even subtle differences in the restoration become visible.

Zirconia Bridge for Front Teeth: Can It Match Porcelain?
For most patients seeking a zirconia bridge for front teeth, modern translucent zirconia is both clinically appropriate and aesthetically excellent. When fabricated in a quality laboratory, it is virtually indistinguishable from natural teeth.
The aesthetic edge of porcelain only becomes meaningful in very specific cases — for example, a single highly visible front tooth that must precisely match unusually translucent adjacent natural teeth. In those situations, your clinician may discuss layered porcelain, lithium disilicate (E-max), or a hybrid option.
The Gum Line Problem — Why Metal-Free Matters
One of the most underappreciated long-term disadvantages of porcelain-fused-to-metal (PFM) bridges is what happens as the gum tissue recedes naturally over years. The dark metal margin at the base of a PFM crown can become visible — creating an unaesthetic grey line at the gingival margin. This is a well-documented clinical reality, particularly for upper front teeth restorations.
Zirconia is entirely metal-free. There is no metal substructure and therefore no metal margin. Even as gum tissue changes over decades, the aesthetics of a zirconia bridge are not compromised by a visible dark border. This is a meaningful long-term aesthetic advantage that many patients are not informed of at the planning stage.
Biocompatibility: Which Material Is Safer for Your Body?
This is an important comparison dimension when discussing zirconia vs porcelain bridge biocompatibility.
Both materials are generally well-tolerated by the human body. However, the distinction is clinically meaningful when PFM bridges are included in the comparison. PFM bridges contain metal alloys such as nickel, chromium, or cobalt — which can trigger localised sensitivity reactions in patients with metal allergies or sensitivities, including gum irritation and, in rare cases, more significant immune responses.
Zirconia is entirely metal-free and has a strong biocompatibility profile. A 2024 clinical comparison found that zirconia surfaces accumulated less bacterial plaque, produced lower gingival inflammation scores, and supported healthier gum tissue — reducing the risk of peri-implantitis-adjacent complications around restoration margins. For patients with known metal sensitivities, zirconia is the clinically recommended choice.
All-ceramic porcelain (without a metal base) is also biocompatible. The biocompatibility distinction applies most directly when comparing zirconia against PFM specifically.

The Honest Disadvantages of Zirconia Bridges
Understanding what are the disadvantages of zirconia bridges is essential for an honest comparison. Zirconia is the superior material in most clinical scenarios — but it is not without limitations.
1. Fracture under extreme force is possible. Zirconia is significantly more fracture-resistant than porcelain, but it can still crack under severe impact or abnormal occlusal loading — particularly in patients with extreme bruxism who do not use a night guard. When zirconia does fracture, it tends to do so catastrophically rather than chip gradually as porcelain does. This is uncommon, but clinically relevant.
2. It may cause enamel wear on opposing natural teeth. Zirconia’s hardness can, in some patients, accelerate enamel wear on opposing teeth. This is more associated with older, higher-density zirconia formulations. Modern translucent zirconia variants have been developed partly to reduce this risk. Your clinician can select the appropriate grade based on your occlusal profile.
3. Aesthetic results are laboratory-dependent. Zirconia’s visual potential is real — but a poorly milled or inadequately characterised zirconia restoration can appear flat and artificial. The clinical outcome depends on the quality of the laboratory and the ceramist. Choosing a clinic with a precision digital fabrication workflow matters significantly.
4. Fractures cannot be repaired chairside. If a small chip occurs on a porcelain surface, it can sometimes be polished or partially repaired in the chair. Zirconia fractures are generally non-repairable in situ and require full restoration replacement.
When Is Porcelain the Better Choice?
Despite zirconia’s growing clinical dominance, there are specific scenarios where porcelain or an all-ceramic alternative remains a legitimate and clinically appropriate option.
- Front teeth with extreme aesthetic demands: When a patient has very thin, highly translucent natural teeth and a single front-tooth pontic must precisely match them, layered porcelain or lithium disilicate may produce a more optically nuanced result than standard zirconia.
- Shorter-span restorations in low-pressure zones: For a 3-unit bridge in a low-stress anterior area where aesthetic nuance is the primary concern, all-ceramic porcelain is a clinically reasonable option.
- Budget-sensitive cases: All-ceramic porcelain bridges carry a lower initial laboratory cost in most markets, though the shorter replacement cycle can offset this advantage over time.
Porcelain is not an inferior material — it is a different material with a different performance profile. The right choice depends on placement zone, bite habits, and aesthetic priorities.
Zirconia vs Porcelain: Head-to-Head Comparison
| Factor | Zirconia | All-Ceramic Porcelain | PFM (Porcelain-Fused-to-Metal) |
|---|---|---|---|
| Fracture Resistance | ★★★★★ 900–1,200 MPa | ★★☆☆☆ 100–400 MPa | ★★★★☆ High (metal core) |
| Strength for Back Teeth | ★★★★★ Ideal | ★★☆☆☆ Risk of fracture | ★★★★☆ Good |
| Natural Appearance | ★★★★☆ Excellent (modern translucent) | ★★★★★ Finest translucency | ★★★☆☆ Moderate |
| Gum Line Aesthetics | ★★★★★ No metal line ever | ★★★★★ No metal line | ★★☆☆☆ Metal margin may show over time |
| Biocompatibility | ★★★★★ Metal-free, low plaque | ★★★★★ Biocompatible | ★★★☆☆ Metal allergy possible |
| Suitable for Front Teeth | ★★★★☆ Excellent | ★★★★★ Optimal in extreme aesthetic cases | ★★★☆☆ Gum margin risk long-term |
| Metal-Free | ✅ Yes | ✅ Yes | ❌ No |
| CAD/CAM Precision | ✅ Yes | Varies | Varies |
| Opposing Tooth Wear Risk | ⚠️ Higher grades may cause wear | ☑️ Lower risk | ☑️ Lower risk |
| Chairside Repair Possible | ❌ Rarely | ✅ Sometimes | ✅ Sometimes |
| Long-term Value | ★★★★★ 15+ years | ★★★☆☆ 5–10 years | ★★★★☆ 10–15 years |
Which Should You Choose? A Decision Guide by Patient Type
There is no universal answer to the zirconia dental bridge vs porcelain question. The right material depends on your specific clinical situation. Here is a practical framework to help you ask better questions at your consultation.
Choose zirconia if:
- Your bridge replaces back teeth or molars
- You clench or grind your teeth (bruxism)
- You have a metal sensitivity or allergy
- You want the lowest long-term maintenance requirement
- You value gum health and metal-free aesthetics over a 10–20 year horizon
- Your bridge is supported on dental implants
Porcelain (all-ceramic) may be worth discussing if:
- Your bridge is in the upper visible anterior zone
- Adjacent natural teeth are very light and highly translucent
- Bite pressure in that area is minimal
- Aesthetic nuance is your absolute top priority and you accept the shorter restoration lifespan
PFM may be relevant if:
- You are replacing a long-span bridge where a metal substructure adds structural benefit
- Your existing bridge is already PFM and you are matching it
- Budget is the primary constraint and durability is secondary
Your clinician’s recommendation should always guide the final decision. These guidelines are designed to help you arrive at your consultation better informed — not to replace a clinical assessment.
Why Are Dentists Increasingly Recommending Zirconia Over Porcelain?
Why are dentists pushing the use of zirconia in modern practice? The shift reflects two converging developments: advances in zirconia material science — particularly translucent zirconia and monolithic zirconia formulations — and the wider availability of precision CAD/CAM manufacturing technology.
Clinicians who previously relied on PFM or layered porcelain have moved toward zirconia because it delivers more consistent long-term outcomes with fewer callbacks for chipping, fracture repair, or gum line aesthetic complaints. As zirconia’s appearance has improved significantly over the past decade, the trade-off between aesthetics and strength that once favoured porcelain in anterior cases has largely closed.
At Kristal Clinic in Istanbul, our restorative team works with an in-house CAD/CAM digital laboratory to produce zirconia bridges with precision milling. If you are comparing your options before your appointment, you can submit your X-ray or CBCT scan for a remote pre-assessment at no cost.
Are Zirconia Bridges Worth the Money?
Are zirconia bridges worth the money? For most patients, yes — with one important qualification.
Zirconia bridges carry a higher initial laboratory cost than porcelain alternatives in most markets. However, the value calculation changes when you factor in the longer service life, lower replacement frequency, and reduced risk of managing complications. A zirconia bridge that functions reliably for 15 or more years with proper care often represents a stronger clinical and financial investment than a porcelain bridge requiring repair or replacement within a shorter timeframe.
There is also a non-financial consideration: the clinical inconvenience of bridge failure. A fractured porcelain bridge can disrupt function, require emergency visits, and in some cases necessitate new impressions and a waiting period for a replacement restoration. Zirconia’s superior fracture resistance reduces — though does not eliminate — this risk.
For patients travelling to Türkiye for dental treatment, where clinical quality and cost efficiency already combine favourably, choosing a more durable material at the point of treatment reduces the need for follow-up interventions after returning home.
For a full breakdown of bridge costs by unit, arch type, and country, see our zirconia bridge cost guide for Türkiye, UK, and USA.
Frequently Asked Questions
Which is better — a zirconia or porcelain fixed bridge?
For most patients, zirconia is the stronger, more durable, and more biocompatible choice. It performs better under occlusal force, is metal-free, and maintains long-term gum line aesthetics. Porcelain remains a valid option in specific anterior aesthetic cases requiring the finest translucency.
What are the disadvantages of zirconia bridges?
Zirconia’s main limitations include its hardness — which can sometimes cause enamel wear on opposing teeth in certain grades — its higher initial cost compared to porcelain, and the fact that fractures cannot typically be repaired chairside and require full restoration replacement.
Can a zirconia bridge break?
Yes, though it is far more fracture-resistant than porcelain. Zirconia can crack under severe force or extreme bruxism without occlusal protection. When it fractures, it tends to do so completely rather than chipping gradually.
What looks more natural — zirconia or porcelain?
Modern translucent zirconia is virtually indistinguishable from natural teeth in the majority of clinical cases. Porcelain retains a narrow aesthetic edge only in very specific situations — when matching extremely light, highly translucent anterior natural teeth. For most patients, zirconia provides an excellent, natural-looking result.
Why are dentists recommending zirconia more than porcelain?
Zirconia’s combination of strength, biocompatibility, metal-free aesthetics, and CAD/CAM manufacturing precision has made it the preferred restorative material in modern dentistry. It delivers more consistent long-term outcomes than older PFM or all-ceramic porcelain options.
Do dentists still use porcelain-fused-to-metal bridges?
PFM bridges are still clinically available and used in specific scenarios — particularly for long-span bridges where a metal substructure adds structural rigidity, or in budget-constrained cases. However, zirconia has replaced PFM as the standard of care in most modern restorative practices.
Summary
The zirconia dental bridge vs porcelain decision is not about which material is universally superior — it is about matching the right material to your clinical situation.
Zirconia is the stronger, more biocompatible, and more aesthetically durable choice for the majority of patients — particularly those needing posterior bridges, those with bruxism, patients with metal sensitivities, and those planning implant-supported restorations. Its metal-free construction, CAD/CAM precision, and long-term gum line integrity make it the default recommendation in modern restorative dentistry.
Porcelain — and specifically high-grade all-ceramic porcelain or lithium disilicate — retains a role in specific aesthetic cases where the finest optical translucency is required for highly visible anterior teeth.
The best starting point is a clinical consultation with a prosthodontist who can evaluate your bite, adjacent tooth condition, gum health, and overall oral profile before recommending a material.
Ready to understand which material is right for your bridge? The clinical team at Kristal Clinic, Istanbul, offers remote pre-assessments for international patients. Share your existing X-ray or dental records and receive a tailored material recommendation before travelling.
→ Request a Free Remote Evaluation
Or explore the full range of bridge designs available at Kristal Clinic — including zirconia, E-max, Maryland, and PFM options — to understand which bridge type suits your case.